What is the only biologic regimen FDA-approved
as 2L treatment for use starting at induction for
women with platinum-sensitive ovarian cancer?
What is the only biologic regimen FDA-approved as 2L treatment for use starting at induction for women with platinum-sensitive ovarian cancer?
A Avastin + chemotherapy
B PARP inhibitors
C Anti-EGFRs
is the only biologic regimen
FDA-approved as 2L treatment
for use starting at induction for
women with psOC
View the studies
- Contact a representative
- Footnotes
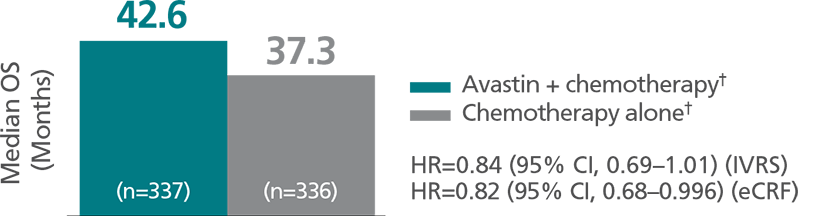
2L=second-line; psOC=platinum-sensitive ovarian cancer; PFS=progression-free survival; HR=hazard ratio; CI=confidence interval; GOG=Gynecologic Oncology Group; OS=overall survival; IVRS=interactive voice response system; eCRF=electronic case report form.
Chemotherapy included carboplatin and gemcitabine.
Chemotherapy included carboplatin and paclitaxel. - Reference
Reference:
1. Avastin Prescribing Information.
Genentech, Inc. 2017.
Avastin plus chemotherapy is the only biologic regimen FDA-approved as 2L treatment for use starting at induction for women with platinum-sensitive ovarian cancer1
OCEANS
Main efficacy outcome
measure: PFS

GOG-0213
Main efficacy outcome
measure: OS
OCEANS
Main efficacy outcome measure: PFS1
GOG-0213
Main efficacy outcome measure: OS1
Boxed WARNINGS
- Gastrointestinal (GI) perforation
- Serious and sometimes fatal GI perforation occurs at a higher incidence in Avastin-treated patients compared to patients treated with chemotherapy
- The incidence of GI perforation ranged from 0.3% to 3% across clinical studies
- Discontinue Avastin in patients with GI perforation
- Surgery and wound healing complications
- The incidence of wound healing and surgical complications, including serious and fatal complications, is increased in Avastin-treated patients
- Withhold Avastin for at least 28 days prior to elective surgery. Do not administer Avastin for at least 28 days after surgery and until the wound is fully healed
- Discontinue in patients with wound healing complications requiring medical intervention
- Hemorrhage
- Severe or fatal hemorrhage, including hemoptysis, GI bleeding, hematemesis, central nervous system hemorrhage, epistaxis, and vaginal bleeding, occurred up to 5-fold more frequently in patients receiving Avastin. In clinical studies, the incidence of grade ≥3 hemorrhagic events among patients receiving Avastin ranged from 0.4% to 7%
- Do not administer Avastin to patients with serious hemorrhage or a recent history of hemoptysis (≥1/2 tsp of red blood)
- Discontinue Avastin in patients who develop grade 3-4 hemorrhage
- Footnotes
2L=second-line; psOC=platinum-sensitive ovarian cancer; PFS=progression-free survival; HR=hazard ratio; CI=confidence interval; GOG=Gynecologic Oncology Group; OS=overall survival; IVRS=interactive voice response system; eCRF=electronic case report form.
Chemotherapy included carboplatin and gemcitabine.
Chemotherapy included carboplatin and paclitaxel. - Reference
Reference:
1. Avastin Prescribing Information.
Genentech, Inc. 2017. - Contact a representative
Scroll for important safety information,
including Boxed WARNINGS.
Please see full Prescribing Information, including Boxed WARNINGS, for additional important safety information.
Indications
Avastin® (bevacizumab) injection, for intravenous use, in combination with paclitaxel, pegylated liposomal doxorubicin, or topotecan, is indicated for the treatment of patients with platinum-resistant recurrent epithelial ovarian, fallopian tube or primary peritoneal cancer who received no more than 2 prior chemotherapy regimens.
Avastin, in combination with carboplatin and paclitaxel, or with carboplatin and gemcitabine, followed by Avastin as a single agent, is indicated for the treatment of patients with platinum-sensitive recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer.
Boxed WARNINGS
-
Gastrointestinal (GI) perforation
- Serious and sometimes fatal GI perforation occurs at a higher incidence in Avastin-treated patients compared to patients treated with chemotherapy
- The incidence of GI perforation ranged from 0.3% to 3% across clinical studies
- Discontinue Avastin in patients with GI perforation
- Surgery and wound healing complications
- The incidence of wound healing and surgical complications, including serious and fatal complications, is increased in Avastin-treated patients
- Withhold Avastin for at least 28 days prior to elective surgery. Do not administer Avastin for at least 28 days after surgery and until the wound is fully healed
- Discontinue in patients with wound healing complications requiring medical intervention
- Hemorrhage
- Severe or fatal hemorrhage, including hemoptysis, GI bleeding, hematemesis, central nervous system hemorrhage, epistaxis, and vaginal bleeding, occurred up to 5-fold more frequently in patients receiving Avastin. In clinical studies, the incidence of grade ≥3 hemorrhagic events among patients receiving Avastin ranged from 0.4% to 7%
- Do not administer Avastin to patients with serious hemorrhage or a recent history of hemoptysis (≥1/2 tsp of red blood)
- Discontinue Avastin in patients who develop grade 3-4 hemorrhage
Additional serious adverse events
- Additional serious and sometimes fatal adverse events with increased incidence in the Avastin-treated arm vs chemotherapy arm included:
- Non-GI fistulae (<1% to 1.8%, highest in patients with cervical cancer)
- Arterial thromboembolic events (grade ≥3, 5%, highest in patients with GBM)
- Renal injury and proteinuria
- Grade 3–4 proteinuria ranged from 0.7% to 7% in clinical studies
- Nephrotic syndrome (<1%)
- Additional serious adverse events with increased incidence in the Avastin-treated arm vs chemotherapy arm included:
- Venous thromboembolism (grade ≥3, 11% seen in GOG-0240)
- Hypertension (grade 3–4, 5%–18%)
- Posterior reversible encephalopathy syndrome (PRES) (<0.5%)
- Congestive heart failure (CHF) (1%)
- Infusion reactions with the first dose of Avastin occurred in <3% of patients, and severe reactions occurred in 0.2% of patients
- Avoid use in patients with ovarian cancer who have evidence of recto-sigmoid involvement by pelvic examination or bowel involvement on CT scan or clinical symptoms of bowel obstruction
- Inform females of reproductive potential of the risk of ovarian failure prior to initiating treatment with Avastin
Pregnancy warning
- Based on the mechanism of action and animal studies, Avastin may cause fetal harm
- Advise female patients that Avastin may cause fetal harm, and to inform their healthcare provider of a known or suspected pregnancy
- Advise females of reproductive potential to use effective contraception during treatment with Avastin and for 6 months after the last dose of Avastin
- Advise nursing women that breastfeeding is not recommended during treatment with Avastin and for 6 months following their last dose of treatment
- Avastin may impair fertility
Most common adverse events
- Across studies, the most common adverse reactions observed in Avastin patients at a rate >10% were:
- Epistaxis
- Headache
- Hypertension
- Rhinitis
- Proteinuria
- Taste alteration
- Dry skin
- Rectal hemorrhage
- Lacrimation disorder
- Back pain
- Exfoliative dermatitis
- Across all studies, Avastin was discontinued in 8% to 22% of patients because of adverse reactions
Indication-specific adverse events
- In psOC, grade 3 or 4 adverse reactions in the OCEANS study occurring at a higher incidence (≥2%) in 247 patients receiving Avastin plus carboplatin and gemcitabine (chemotherapy), compared to 233 patients receiving placebo plus chemotherapy, were thrombocytopenia (40% vs 34%), nausea (4% vs 1.3%), fatigue (6% vs 4%), headache (4% vs 0.9%), proteinuria (10% vs 0.4%), dyspnea (4% vs 1.7%), epistaxis (5% vs 0.4%), and hypertension (17% vs 0.9%)
- In psOC, grade 3 or 4 adverse reactions in the GOG-0213 study occurring at a higher incidence (≥2%) in 325 patients receiving Avastin plus carboplatin and paclitaxel (chemotherapy), compared to 332 patients receiving chemotherapy alone, were hypertension (11% vs 0.6%), fatigue (8% vs 3%), febrile neutropenia (6% vs 3%), proteinuria (8% vs 0%), abdominal pain (6% vs 0.9%), hyponatremia (4% vs 0.9%), headache (3% vs 0.9%), and pain in extremity (3.4% vs 0%)
- In prOC, grade 3–4 adverse reactions in AURELIA occurring at a higher incidence (≥2%) in 179 patients receiving Avastin plus chemotherapy, compared to 181 patients receiving chemotherapy alone, were hypertension (6.7% vs 1.1%) and palmar-plantar erythrodysaesthesia syndrome (4.5% vs 1.7%)
You may report side effects to the FDA at (800) FDA-1088 or www.fda.gov/medwatch.
You may also report side effects to Genentech at (888) 835-2555.
Please see full Prescribing Information, including Boxed WARNINGS, for additional important safety information.
AVY/010318/0001 (03/18)
![]()