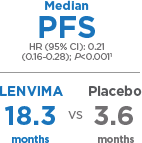
PFS=progression-free survival; HR=hazard ratio; CI=confidence interval.
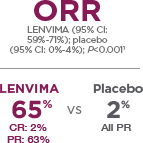
ORR=objective response rate; CR=complete response; PR=partial response.
LENVIMA was studied in the SELECT Trial (Study of [E7080] LEnvatinib in Differentiated Cancer of the Thyroid), a multicenter, randomized (2:1), double-blind, placebo-controlled trial conducted in 392 patients with locally recurrent or metastatic radioactive iodine-refractory differentiated thyroid cancer (RAI-refractory DTC) and radiographic evidence of disease progression within 12 months prior to randomization, confirmed by independent radiologic review. RAI-refractory was defined as 1 or more measurable lesions with no iodine uptake on RAI scan, iodine uptake with progression within 12 months of RAI therapy, or having received cumulative RAI activity of >600 mCi (22 GBq) with the last dose administered at least 6 months prior to study entry.1
Patients were randomized to receive LENVIMA 24 mg once daily (n=261) or placebo (n=131) until disease progression. Randomization was stratified by geographic region, prior vascular endothelial growth factor/vascular endothelial growth factor receptor-targeted therapy, and age. The primary end point was PFS, as determined by blinded, independent, radiologic review using Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1. Independent review confirmation of disease progression was required prior to discontinuing patients from the randomization phase of the study. Secondary end points included ORR and overall survival. Patients in the placebo arm could receive LENVIMA following independent review confirmation of disease progression.1
Learn more
about
LENVIMA.
 LENVIMA® is a registered trademark used by Eisai Inc. under license from Eisai R&D Management Co., Ltd.
LENVIMA® is a registered trademark used by Eisai Inc. under license from Eisai R&D Management Co., Ltd.
© 2016 Eisai Inc. All rights
reserved. August 2016
LENVIMA.com/hcp
LENV-US0436a
Indication
LENVIMA® (lenvatinib) is indicated for the treatment of patients with locally recurrent or metastatic, progressive, radioactive iodine-refractory differentiated thyroid cancer (RAI-refractory DTC).
Important Safety Information
Warnings and Precautions
- Hypertension was reported in 73% of patients on LENVIMA vs 16% with placebo (44% vs 4% grade ≥3). Blood pressure should be controlled prior to treatment and monitored throughout. Withhold dose for grade 3 hypertension despite optimal antihypertensive therapy; resume at reduced dose when controlled at grade ≤2. Discontinue for life-threatening hypertension
- Cardiac dysfunction was reported in 7% of patients on LENVIMA vs 2% with placebo (2% vs 0% grade ≥3). Monitor for signs/symptoms of cardiac decompensation. Withhold for grade 3 cardiac dysfunction. Resume at reduced dose or discontinue based on severity and persistence of cardiac dysfunction. Discontinue for grade 4 cardiac dysfunction
- Arterial thromboembolic events were reported in 5% of patients on LENVIMA vs 2% with placebo (3% vs 1% grade ≥3). Discontinue following an arterial thrombotic event. The safety of resuming LENVIMA after an arterial thromboembolic event has not been established, and LENVIMA has not been studied in patients who have had an arterial thromboembolic event within the previous 6 months
- Across clinical studies in which 1,160 patients received LENVIMA monotherapy, hepatic failure (including fatal events) was reported in 3 patients and acute hepatitis in 1 patient. ALT and AST increases (grade ≥3) occurred in 4% and 5% of patients on LENVIMA, respectively, vs 0% with placebo. Monitor liver function before initiation, then every 2 weeks for the first 2 months, and at least monthly thereafter during treatment. Withhold dose for liver impairment grade ≥3 until resolved to grade 0, 1, or baseline. Resume at reduced dose or discontinue based on severity/persistence of hepatotoxicity. Discontinue for hepatic failure
- Proteinuria was reported in 34% of patients on LENVIMA vs 3% with placebo (11% vs 0% grade 3). Monitor for proteinuria before and during treatment. Withhold dose for proteinuria ≥2 g/24 h. Resume at reduced dose when proteinuria is <2 g/24 h. Discontinue for nephrotic syndrome
- Events of renal impairment were reported in 14% of patients on LENVIMA vs 2% with placebo (3% vs 1% grade ≥3). Withhold LENVIMA for grade 3 or 4 renal failure/impairment. Resume at reduced dose or discontinue, depending on severity/persistence of renal impairment. Active management of diarrhea and any other gastrointestinal (GI) symptoms should be initiated for grade 1 events
- Events of GI perforation or fistula were reported in 2% of patients on LENVIMA vs 0.8% with placebo. Discontinue in patients who develop GI perforation or life-threatening fistula
- QT/QTc interval prolongation was reported in 9% of patients on LENVIMA vs 2% with placebo (2% vs 0% >500 ms). Monitor electrocardiograms in patients with congenital long QT syndrome, congestive heart failure, bradyarrhythmias, or patients taking drugs known to prolong the QT interval. Monitor and correct electrolyte abnormalities in all patients. Withhold dose for QTc interval prolongation >500 ms. Resume at reduced dose when QTc prolongation resolves to baseline
- Hypocalcemia (grade ≥3) was reported in 9% of patients on LENVIMA vs 2% with placebo. Monitor blood calcium levels at least monthly and replace calcium as necessary. Interrupt and adjust LENVIMA as necessary
- Across clinical studies in which 1,160 patients received LENVIMA monotherapy, reversible posterior leukoencephalopathy syndrome (RPLS) was reported in 4 patients. Withhold LENVIMA for RPLS until fully resolved. Resume at reduced dose or discontinue based on the severity and persistence of neurologic symptoms
- Hemorrhagic events occurred in 35% of patients on LENVIMA vs 18% with placebo (2% vs 3% grade ≥3). The most frequently reported hemorrhagic event was epistaxis (11% grade 1, 1% grade 2). Discontinuation due to hemorrhagic events occurred in 1% of patients on LENVIMA. There was 1 fatal intracranial hemorrhage case among 16 patients who received LENVIMA and had central nervous system metastases at baseline. Consider the risk of severe or fatal hemorrhage associated with tumor invasion/infiltration of major blood vessels (eg, carotid artery). Withhold dose for grade 3 hemorrhage. Resume at reduced dose or discontinue based on severity/persistence of hemorrhage. Discontinue for grade 4 hemorrhage
- In patients with normal baseline thyroid-stimulating hormone (TSH), elevation of TSH level above 0.5 mU/L was observed postbaseline in 57% of patients on LENVIMA vs 14% with placebo. Monitor thyroid function prior to treatment initiation and monthly thereafter. Treat hypothyroidism according to standard medical practice to maintain a euthyroid state
- LENVIMA can cause fetal harm when administered to a pregnant woman. Advise females of reproductive potential to use effective contraception during treatment with LENVIMA and for at least 2 weeks following completion of therapy
Adverse Reactions
- The most common adverse reactions observed in LENVIMA-treated patients vs placebo-treated patients were hypertension (73% vs 16%), fatigue (67% vs 35%), diarrhea (67% vs 17%), arthralgia/myalgia (62% vs 28%), decreased appetite (54% vs 18%), weight decrease (51% vs 15%), nausea (47% vs 25%), stomatitis (41% vs 8%), headache (38% vs 11%), vomiting (36% vs 15%), proteinuria (34% vs 3%), palmar-plantar erythrodysesthesia syndrome (32% vs 1%), abdominal pain (31% vs 11%), and dysphonia (31% vs 5%)
- Adverse reactions led to dose reductions in 68% of patients receiving LENVIMA and in 5% of patients receiving placebo; 18% of patients discontinued LENVIMA and 5% discontinued placebo for adverse reactions. The most common adverse reactions (≥10%) resulting in dose reductions of LENVIMA were hypertension (13%), proteinuria (11%), decreased appetite (10%), and diarrhea (10%); the most common adverse reactions (≥1%) resulting in discontinuation of LENVIMA were hypertension (1%) and asthenia (1%)
Use in Specific Populations
- Because of the potential for serious adverse reactions in nursing infants, advise women to discontinue breastfeeding during treatment
- LENVIMA may result in reduced fertility in females of reproductive potential and may result in damage to male reproductive tissues, leading to reduced fertility of unknown duration
Please see full Prescribing Information at LENVIMA.com/hcp.
Reference: 1. LENVIMA [package insert]. Woodcliff Lake, NJ: Eisai Inc.; 2016.